Healthcare
CLOGS
30 January 2026
From daily symptoms to meaningful health trends and resources
Test out the Hackathon MVP today - https://clogs.site/
If you're interested in chatting with us about this project: https://form.gov.sg/69819f612a982c5ed2848759
The tool followed a simple 'Track, get trends, apply advice' structure on a daily, weekly and monthly basis.
Many families in Singapore rely on foreign domestic workers (FDWs) to support elderly loved ones at home, including during serious illness and end-of-life care. These caregivers often spend the most time with patients day to day, yet have little structured support to recognise what matters, communicate changes clearly, or know when to raise a concern.
Over the past month, we explored how changes in health, comfort, and wellbeing are noticed and acted upon in home caregiving contexts. We focused on helping caregivers (including FDWs) notice early signs that things are getting worse, without turning them into clinicians or increasing their burden.
Rather than formal training, this work centres on structured observation, shared language, and knowing when to raise a concern. The goal is to help caregivers capture what they already see in ways families and clinicians can act on.
Opportunity: Why this matters
Palliative care in Singapore is often introduced late. While 70–80% of people who die would benefit from palliative care, only about 40% receive it, typically very close to death. A major contributor is that early signs of decline at home are missed, normalised, or not raised in time.
Families and FDWs may notice changes like fatigue, pain, confusion, or emotional distress, but these observations are informal, inconsistently communicated, and hard for clinicians to act on between appointments.
Across interviews, we saw a consistent pattern:
Caregivers already observe and track informally, but without structure
Judgement-heavy moments ("should I be worried?") are the hardest to navigate
Clinicians have little visibility into what happens between visits
This matters in a rapidly ageing society where most older adults prefer to age at home and serious illness is increasingly managed in households. When early signs are missed, the cost is human: avoidable distress, crisis hospitalisations, and loss of dignity.
Supporting Data
Demographic scale & ageing
Singapore’s population is rapidly ageing, as of mid-2025, about 18.8% of the resident population is aged 65 and over, and this figure is projected to grow to nearly 1 in 4 by 2030 (~23.9%).
Most older adults prefer to age in place (at home) rather than move to an institution. One study found that 82.8% of older adults prefer to remain in their own homes as they age.
Caregiving burden and context
In Singapore, unpaid caregiving is common: research shows that 1 in 7 older adults is also a caregiver for someone else, often while juggling work and their own health.
A large number of Singaporean caregivers experience burden and stress, with studies showing a significant proportion meeting criteria for moderate to severe caregiver burden.
Caregivers often rely on secondary help, and about 68.6% of primary informal caregivers are assisted by secondary caregivers, most commonly migrant domestic workers (MDWs).
Palliative care landscape
Singapore’s Ministry of Health is expanding home palliative care capacity to about 3,600 places by 2025 (a 50% increase) to support more people at home before and at end of life.
Services like the Equipment Rental Scheme are expected to benefit more than 12,000 Singaporeans on home palliative care over the next three years.
What success would look like
We are still refining how best to measure impact and what the baselines are, but early discussions point to three meaningful indicators:
Caregivers and FDWs feel more confident noticing and raising concerns, without guessing or overstepping.
Clinicians receive earlier, clearer signals that help them respond sooner.
Care outcomes improve through earlier action and fewer last-minute crises.
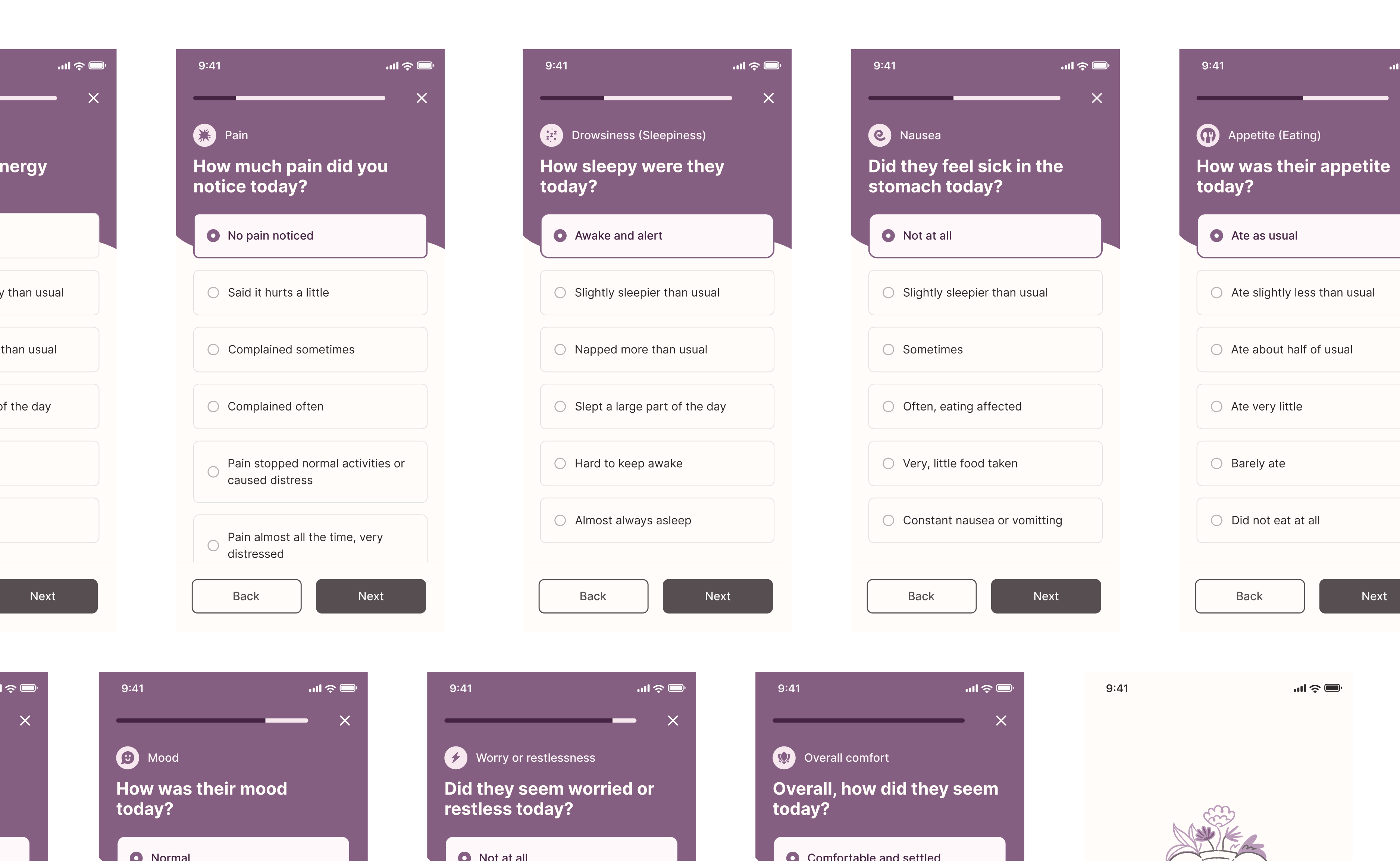
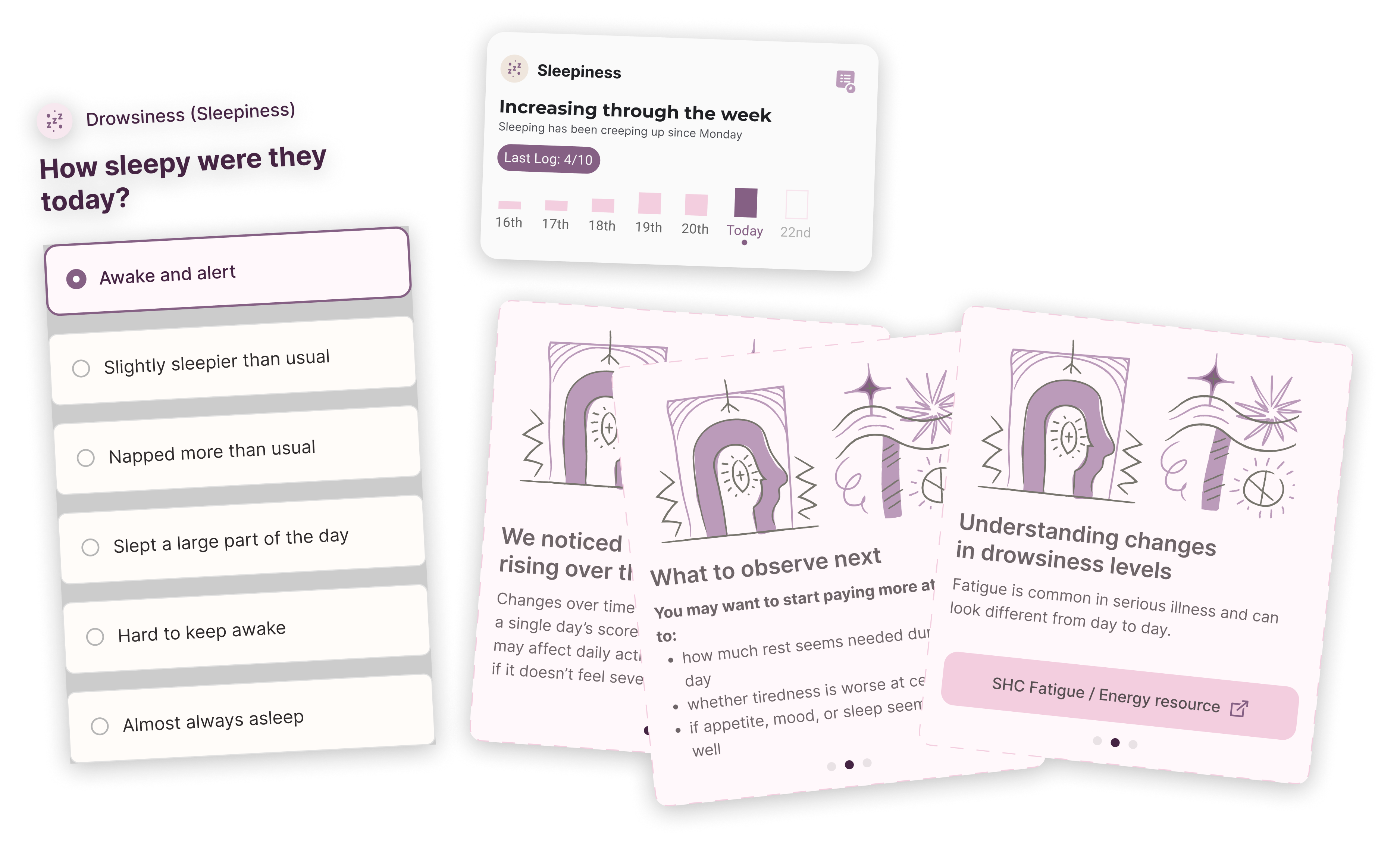
Caregivers captured 9 symptoms on a 0-5 scale everyday, expressed in simpler terms to reduce abstraction.
Velocity: What we built and learned
Over the past month, we conducted 9 interviews across 3 stakeholder groups: 2 FDWs currently in active caregiving roles, 5 family caregivers with direct home palliative experience, and 2 palliative care clinicians (including an emergency department consultant with experience in end-of-life care). We also visited the Singapore Hospice Council early in the process to test our assumptions with their team.
From those conversations, we developed and tested caregiver logging prototypes. We designed simple, non-clinical prompts that reflect real home observations, added helpful guidance without replacing professional judgement, and simplified language across multiple rounds based on caregiver feedback.
Key learnings:
Structure reduces the mental and emotional weight on caregivers
Judgement ("is this concerning?") is harder than doing the task itself
Logging only works if someone is clearly responsible for responding
Standalone tools risk shifting burden onto caregivers
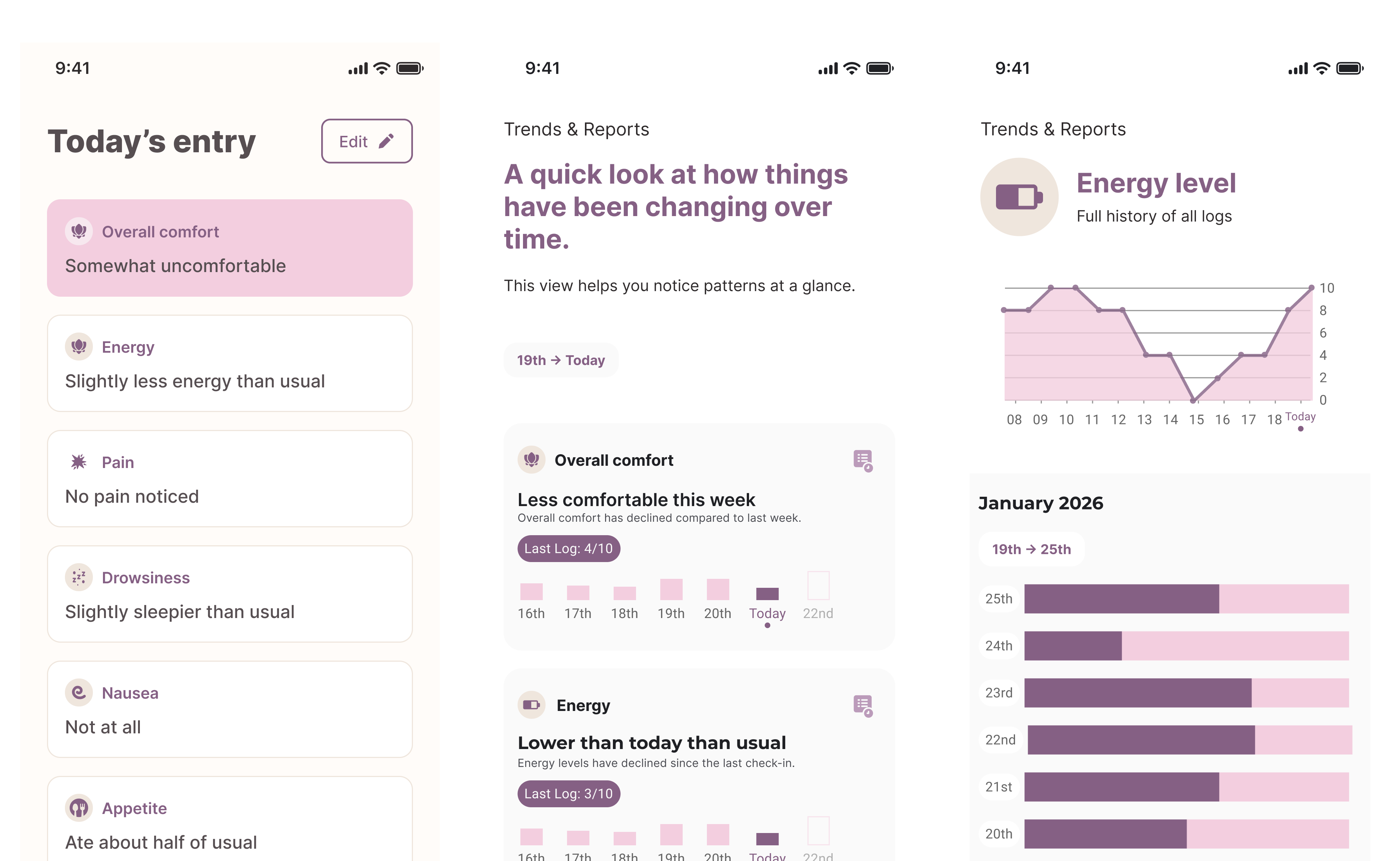
All data was showcased in both a long form timeline and week by week breakdown
Traction: Early signals from real users
We ran a 1-week pilot with 5 caregivers (4 family caregivers and 1 FDW in an active caregiving role) logging daily symptoms for elderly family members at home.
Completion and usability:
4 out of 5 (80%) completed the full week of daily logging
Caregivers self-reported completing each daily log in under 3 minutes, describing the flow as intuitive
What changed in practice: The structured prompts shifted the quality of caregivers' daily conversations, moving from vague check-ins ("how are you feeling?") toward specific, observable questions ("how much did you eat today?", "how much pain did you feel?"). One caregiver piloting the app during her mother's hospitalisation for chemotherapy noted the logs gave her new language to describe what she was seeing, even in a clinical setting.
What clinicians valued: Both clinicians we consulted confirmed that seeing gradual symptom trends over days was more useful than one-off updates. One highlighted opioid dosage frequency and the ability to see patterns between visits as particularly valuable.
Where it fell short: Mid-pilot feedback flagged specific language barriers for non-native English speakers. We simplified prompt phrasing and reduced abstraction in response, which noticeably improved comprehension for the FDW in the group. A consistent tension also emerged: educational resources surfaced after logging felt too generic for more experienced caregivers, suggesting the tool needs to adapt to different levels of caregiver knowledge.
What's next: Closing the gap between visits
Right now, what happens between a clinician's home visit and the next one is largely invisible. Consider this scenario: a clinician visits Mdm Tan on Monday and adjusts her pain medication. Over the following days, her FDW Rina notices she's eating less, sleeping more in the daytime, and seems confused in the evenings. Rina isn't sure if this is normal after a medication change or something the doctor should know about. She mentions it to the family over WhatsApp, but no one is sure what to do. By the time the next visit happens on Friday, Mdm Tan's condition has deteriorated enough that she's sent to the emergency department.
This is the gap Clogs is designed to close. Our pilot showed that structured logging helps caregivers notice and name changes. But it also showed the limits of a one-size-fits-all symptom list. The most useful signals weren't generic. They were specific to the patient's condition and stage of care.
The next phase tests whether that specificity can be built in from the start: after a home visit, a clinician selects a small set of observations tailored to that patient. Not a fixed list of 9 symptoms, but the 3 or 4 things that matter most right now. The caregiver logs against those. The clinician sees the trend before the next visit.
We don't yet know if this works at that level of detail. The next phase is about finding out, through case walkthroughs with clinicians, caregiver reflection sessions, and honest assessment of whether what surfaces is actually useful. If it is, the model could fit into how home palliative care already works in Singapore. If it isn't, we'll say so.